![Premium HIFU Treatment with ‘ULTRAcel [zíː]’](https://joa.jeisys-inc.com/_app/wp-content/uploads/2024/03/JOA_ClinicalBlog_sugino-1-1800x1000.jpg)
Hiroko Sugino, M.D, PhD.
Director, Aoyama Elu Clinic
1. Principle of HIFU
Application of ultrasound in medical settings
High intensity focused ultrasound (HIFU) is a minimally invasive medical procedure that uses ultrasound to heat or ablate tissue. When HIFU is used for aesthetic medical purposes, the ultrasound intensity is lower and its frequency is higher than that used for therapeutic purposes, such as prostate cancer treatment. With this approach, HIFU for aesthetic use can generate heat in a more targeted region. HIFU is emitted from a circular concave transducer and focused a fixed distance (Figure 1). This causes the ultrasonic vibration to create dotted frictional heat in the tissue. It has been designed so that 70% of the heat is generated at the top and 30% at the bottom. As the transducer moves along a straight line and focuses evenly, the tissue shrinks with heat.
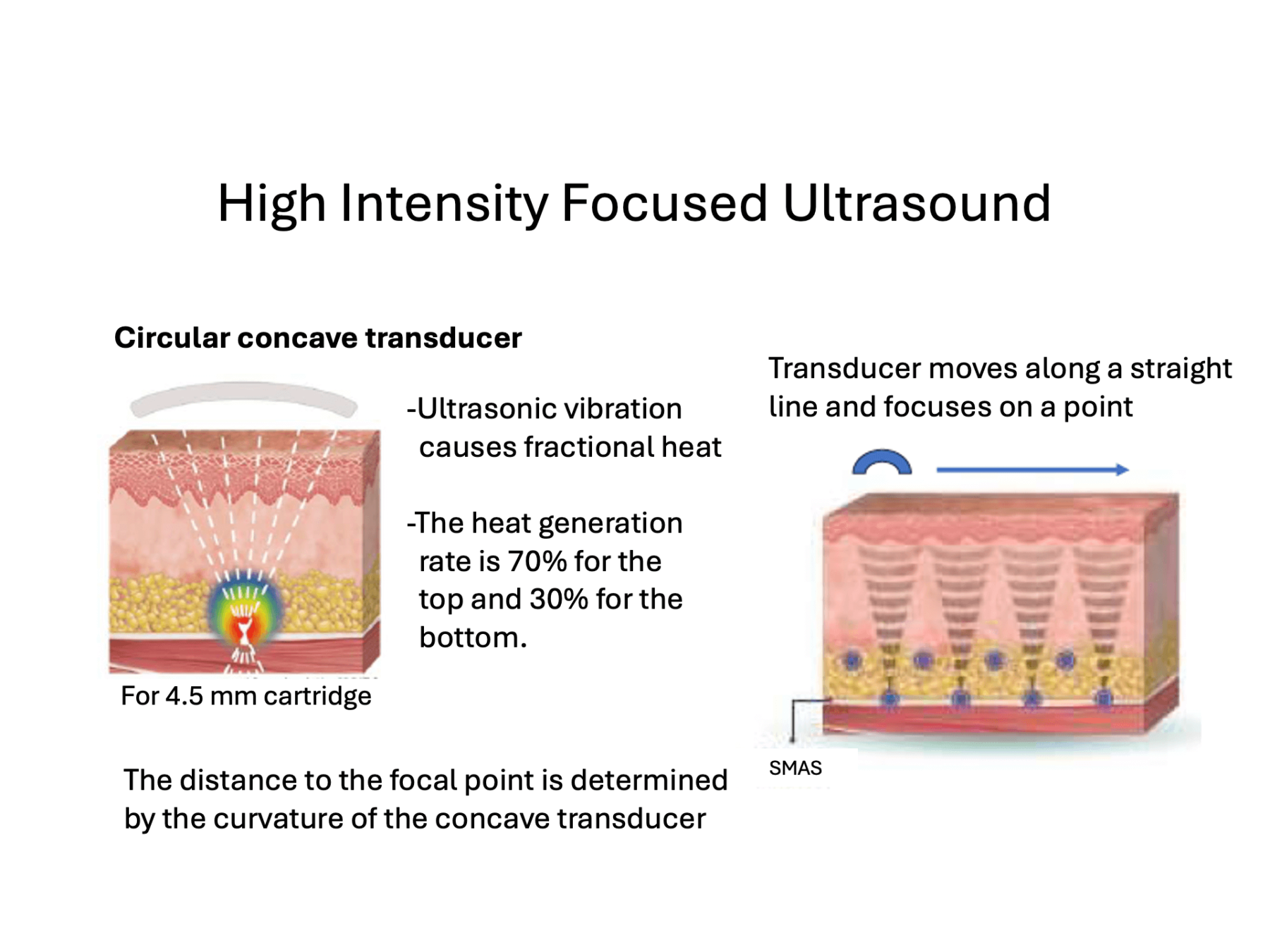
Figure 1. Principle of heat generation in ultrasound
2. History of ULTRAcel
Transition in ULTRAcel Series (2014 – 2023)
In 2014, the first generation ULTRAcel came onto the market. This device incorporated HIFU, radiofrequency (RF), needle radiofrequency, and non-needle radiofrequency hand pieces, and is a multifunction device capable of all-layered therapy from the epidermis to the SMAS layer. HIFU produces heat of 60 °C or more in a dot-like manner, causing strong thermal contraction of collagen. In our clinic, we used to perform radiofrequency treatment together with HIFU to create bulk heating (heat accumulation) over the skin and subcutaneous tissues, achieving effective treatment of sagging. In 2018, the second generation ULTRAcel Q+ was introduced. With this device, the transducers move through the probe at high speed, resulting in a significantly faster irradiation rate. However, I found that treatment with dot HIFU alone was slightly less effective because this version no longer had a radiofrequency probe. Subsequently, when LinearFirm, a HIFU linear irradiation cartridge, was launched on the market, bulk heating also became possible using the ULTRAcel Q+. Currently, the third generation LINEAR Z/ULTRAcel [zi:] (Figure 2) has been introduced. This device enables physicians to switch the focus depth and modes without changing the cartridge. This has improved operability, allowing efficient heating from the dermis to the SMAS layer.
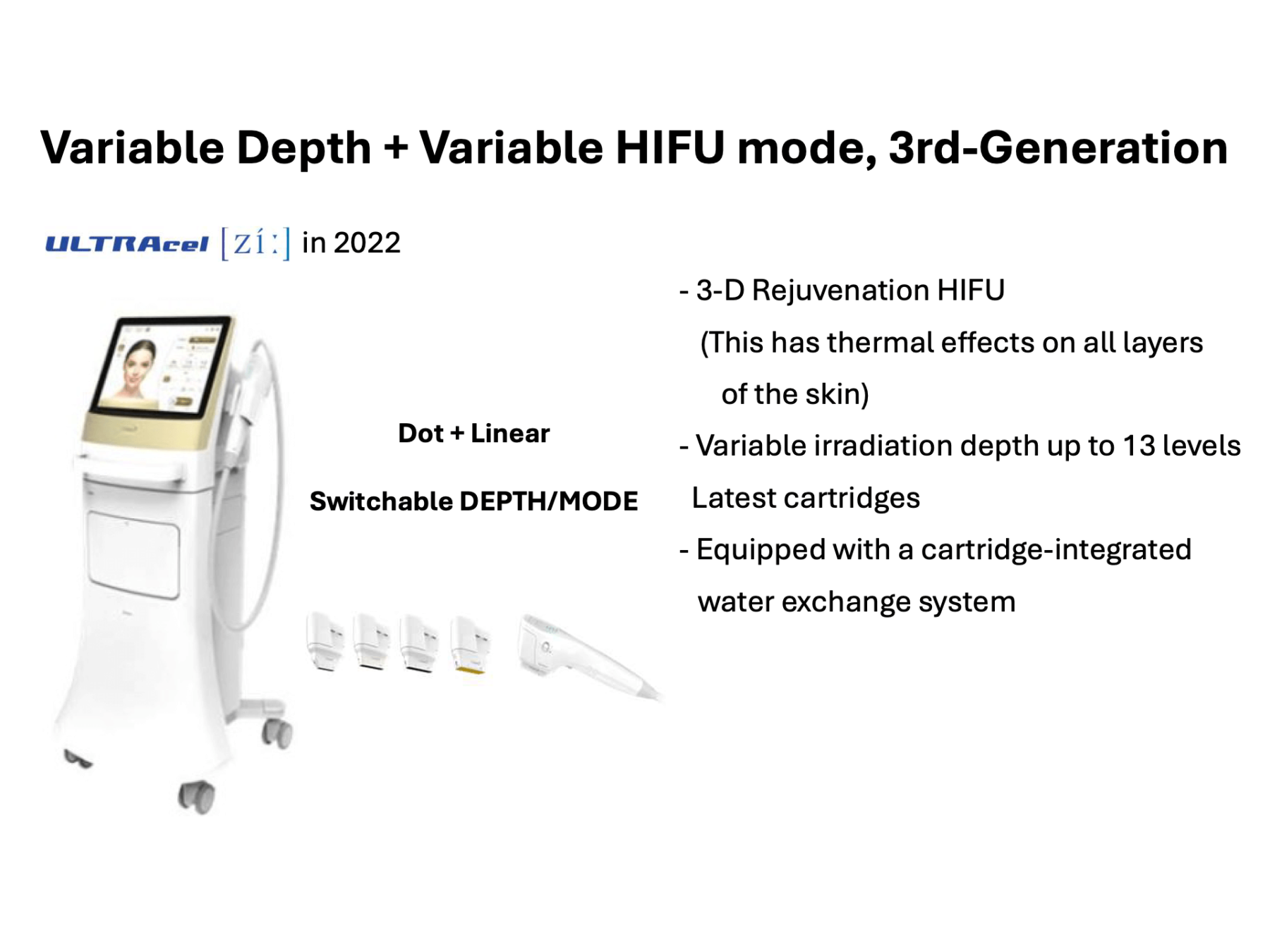
Figure 2. ULTRAcel enters its 3rd generation
In dot mode, the third-generation ULTRAcel can perform lifting and tightening (Figure 3). In linear mode, the system can reduce fat volume by destroying subcutaneous adipocytes through bulk heating. As a result, facial contouring can be achieved. The focal length of the LINEAR Z/ULTRAcel [zi:] can be set to a width of 0.5 mm, which is finer than that of earlier versions. The temperature inside the cartridges is indicated by LEDs. The system allows physicians to switch between the dot and linear modes and to change the focal length with a single action. It also allows physicians to treat the face and even the body by simply preparing four different cartridges. However, it can only be used on the body and not on the face when the focal length is 5 mm or more.
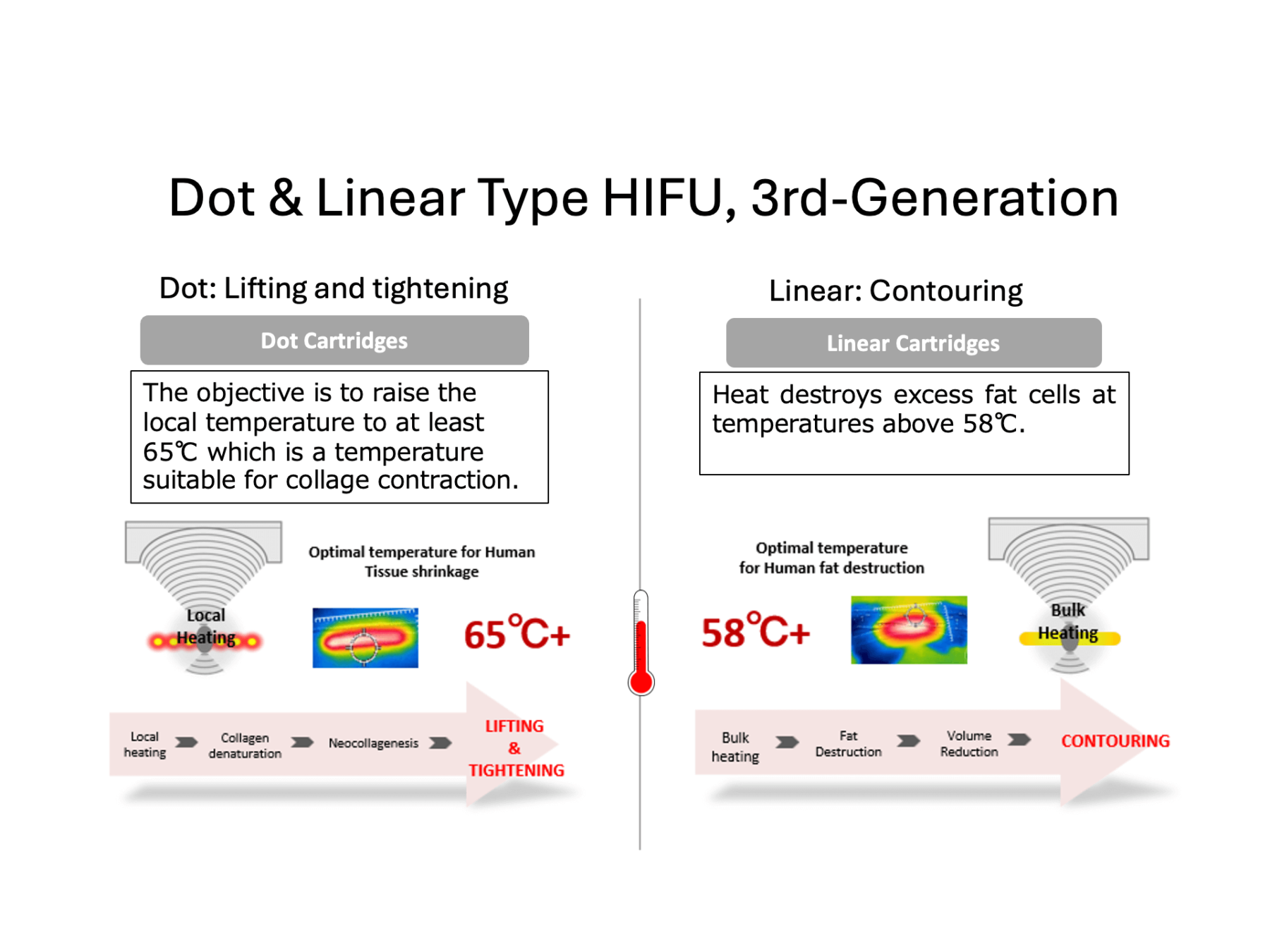
Figure 3. Combination treatment of dot and linear type HIFU enables more customized treatment.
3. Our Treatment Techniques
Usage distinction between the techniques of dot heating and bulk heating
Since the introduction of the first generation ULTRAcel, our clinic has been developing treatment techniques along with the evolution of ULTRAcel. Our basic treatment technique is to perform dot heating and bulk heating simultaneously. We use the latest LINEAR Z/ULTRAcel [zi:] for dot and linear combination treatment based on the same concept as that of the previous model (Figure 4). Dot heating is used to lift the skin by precisely heating each layer, while bulk heating is used to tighten the skin by creating a pool of heat in the skin and subcutaneous tissues.

Figure 4. How to apply heat with dot and bulk heating
The skin contains a network of loose connective tissue that extends from the epidermis to the dermis, subcutaneous fat and fascia. One of the causes of sagging includes weakening of this connective tissue network due to aging. Thus, it is very important to perform bulk heating to thermally denature and rebuild weakened loose connective tissues when treating sagging. Bulk heating is similar to low-temperature cooking; ingredients can be completely cooked at a relatively low temperature for a long period of time. In our clinic, the LINEAR Z/ULTRAcel [zi:] treatment has been performed with 1,000 lines. This number of lines is increased by 40% compared to our conventional treatment. In skin lifting with 500 lines, 4.5 mm, 3.0 mm and 1.5 mm dot mode heating is used. In contouring with 500 lines, by increasing dermal collagen and decreasing subcutaneous fat, 1.5 mm, 3.0 mm, and 4.5 mm linear or dot mode heating is used. These techniques are customized according to the individual condition of the patient.
Our cases
Figure 5 shows a case in which treatment with the ULTRAcel Q+ dot and monopolar radiofrequency treatment with ULTRAcel were performed simultaneously. In this case, the contour of the lower half of the face appears tightened. The entire face also appears slightly slimmed one month after the treatment. The arrows in the 3-D analysis view indicate the distance and direction of hair follicle movement. The hair follicles can be seen moving upward and outward both immediately and one month after the treatment. On the right hemifacial surface, the hair follicles moved by a maximum of 3.1 mm and 2.8 mm immediately and one month after the treatment, respectively; on the left hemiface, hair follicles moved by a maximum of 3.9 mm and 2.8 mm immediately and one month after the treatment, respectively.


Figure 5. Simultaneous treatment with ULTRAcel Q+ Dot and ULTRAcel monopolar radiofrequency
Figure 6 shows a case in which a total of 1200 lines were irradiated with LINEAR Z/ULTRAcel [zi:], skin lifting with dot mode and bulk heating with linear mode using 4.5 mm and 2.0 mm cartridges. Immediately after treatment, it appears that the midface is lifted and the lower half of the face is tightened. It also appears that the nasolabial fold is slightly flattened and the submandibular area is tightened. In addition, the comparison between before and immediately after treatment in 3-D analysis shows an overall lifting effect as well as a displacement of the hair follicles of approximately 5 mm, especially in the preauricular area. The volume changes before and after the treatment show a decrease in the lower part of the nasolabial mounds and the front of the jowls and a slight increase in the volume of the bilateral sub-zygomatic areas.

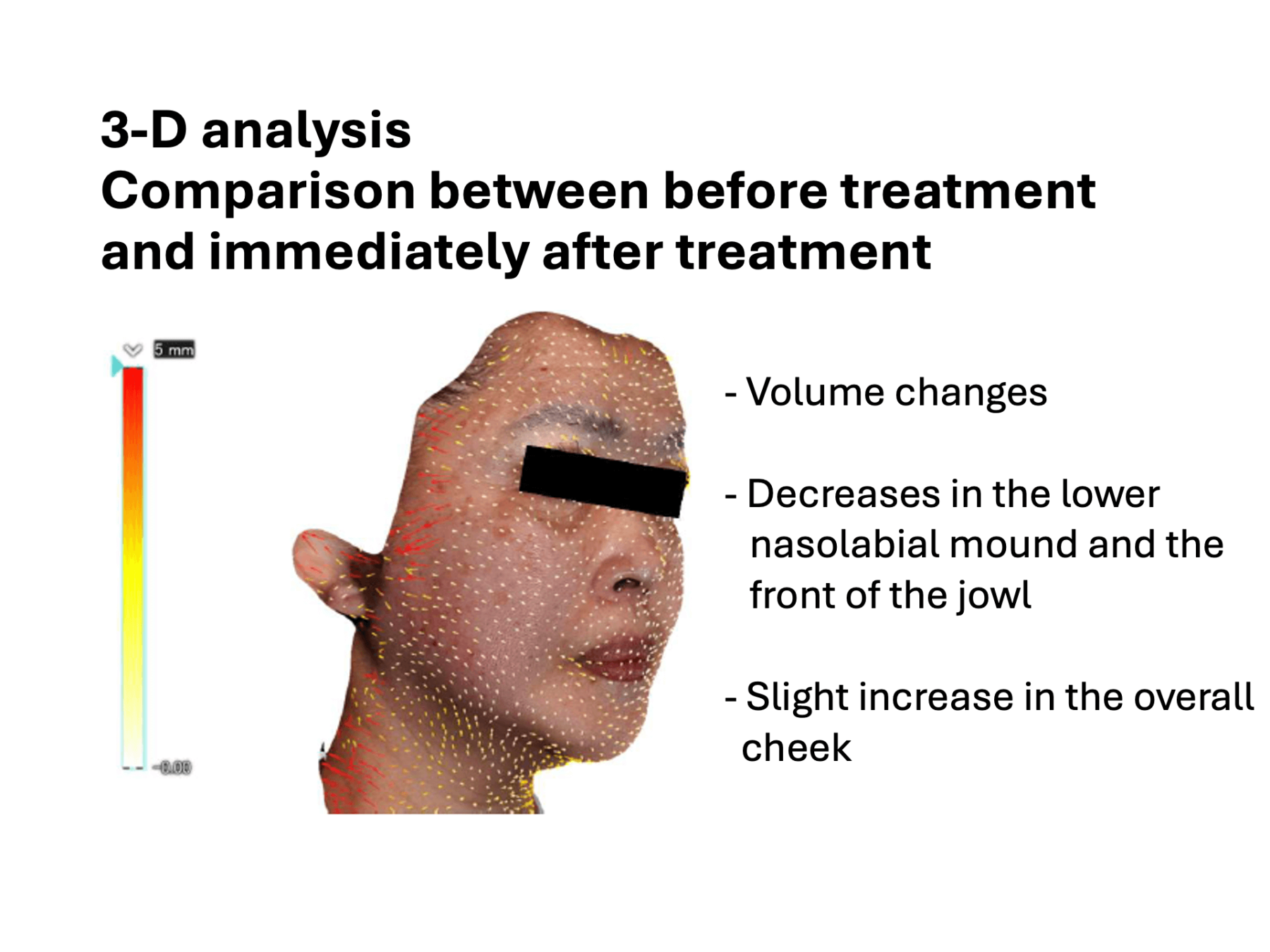
Figure 6. A case where skin lifting was performed in dot mode and bulk heating was performed in linear mode using LINEAR Z/ULTRAcel [zi:] with 4.5 mm and 2.0 mm cartridges.
Treatment of sagging skin is also popular in the upper and lower eyelid area with HIFU. This HIFU treatment with a special periocular probe targets the frontal and temporal areas, sub-eyebrow areas, and lower eyelids. Patients should wear eye shields to protect the eyeballs during this treatment.
4. New Applications of HIFU
Induction of fat loss and fat gain with HIFU
Recent research on contouring with HIFU has focused on the potential application of HIFU to reduce or increase subcutaneous fat. In an experimental study, HIFU was applied to the subcutaneous fat layer of rats fed a high-fat diet to evaluate changes in subcutaneous fat thickness. This study showed that when HIFU was set to 7 MHz, 3.0 mm, 0.6 J/m2 in dot mode, the subcutaneous fat layer thickness gradually decreased even when HIFU did not cause cell necrosis. The study also revealed that heat generated by HIFU can induce p53 gene-dependent apoptosis in the mitochondria and nucleus, as well as cell apoptosis and autophagy. The submandibular area and the jowls are areas where the volume of subcutaneous fat tends to increase with aging. Volume reduction of these areas with HIFU may result in a good contour. In our case shown in Figure 7, we treated the jowls and submandibular areas in linear mode twice with a 2-week interval between treatments. Subsequently, the volume of the submandibular area and the volume of both jowls were reduced; the areas appear to be tightened.

Figure 7. Case of a woman in her 50s
HIFU operating in linear mode has also been used to treat mild orbital fat extrusion in the lower eyelid for which there was no effective treatment other than surgery; this treatment allowed us to reduce the volume of fat slightly.
Meanwhile, a recent study has reported that low-intensity HIFU irradiation increases fat volume (Figure 8).
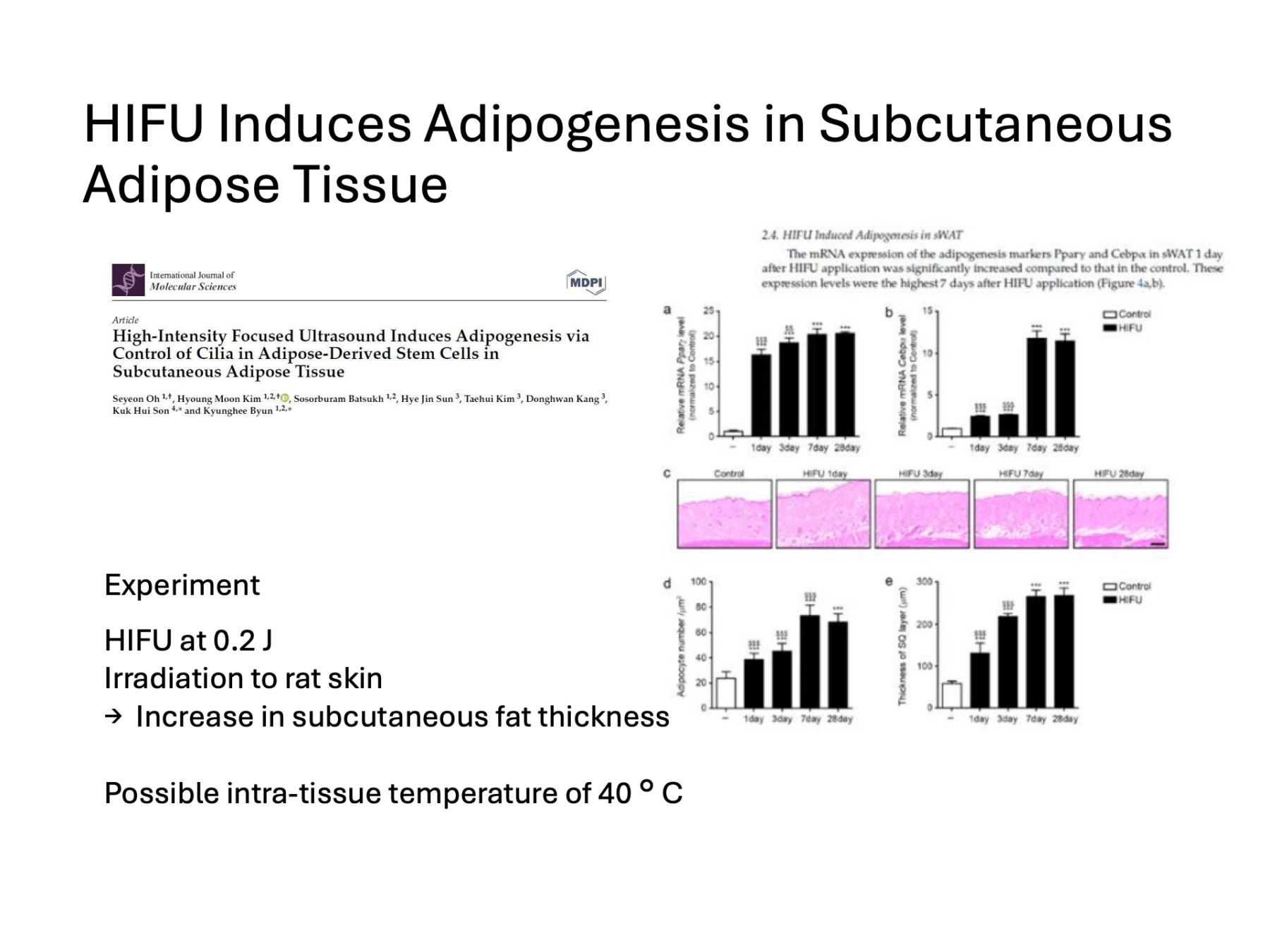
Figure 8. Study of adipogenesis in subcutaneous fat
HIFU has been reported to reduce inflammatory cytokines and regulate the cilia of adipose stem cells to increase subcutaneous adipocytes. The temporal area and lateral cervical sub-zygomatic area are known to lose subcutaneous adipose cells with aging; however, an increase in the subcutaneous fat with HIFU may enable us to achieve a good contour. Based on the results of these studies, new irradiation conditions for HIFU have been proposed (Figure 9). We expect many physicians to try and validate HIFU treatment under these conditions.

Figure 9. New irradiation conditions for HIFU
5. Precautions for Safe Treatment
Precautions in HIFU treatment.
Finally, this paper describes the side effects and their causes, as well as precautions for HIFU treatment. Recently, the Consumer Affairs Agency issued a consumer alert regarding HIFU in aesthetic medical settings. The alert provides an easy-to-understand explanation of the risks of HIFU (e.g. skin disorders, burns, nerve damage leading to paralysis, numbness, and acute cataract), so we recommended that it be read thoroughly. On the other hand, a shocking newspaper article: “Aesthetic Ultrasound Causes Cataract” was published last year. According to this article, a 47-year-old woman presented with sudden loss of vision in her left eye and was diagnosed with acute cataract shortly after undergoing HIFU lid tightening at a beauty salon. The patient subsequently underwent lens surgery and fortunately has regained her vision. The eyelid is the part of the body where the skin is the thinnest. An ultrasound tomogram of the eyelid shows that the thickness of the upper eyelid is only about 1.5 mm. Beneath the skin surface of the eyelid are the subcutaneous tissue, orbicularis oculi muscle, levator palpebrae aponeurosis and Muller’s muscle, tarsus, and conjunctiva. Beneath the conjunctiva are other important tissues, such as the cornea, iris, lens, and vitreous body. Naturally, heating of these tissues has a significant impact on visual acuity; therefore, direct HIFU irradiation of the upper eyelid is contraindicated (Figure 10).

Figure 10. Precautions when exposing the eyelid to HIFU
Side effects to be noted and precautions for the procedure
Skin burns are the most commonly reported side effect of HIFU. There is a risk of focusing on shallow areas of skin on uneven surfaces; therefore, always ensure that the probe is in close contact with the skin surface during irradiation. If a part of the probe is not in close contact, the direction of the probe should be changed. If the gel applied to the skin is too thick and the probe lifts off the skin, the risk of burns increases because HIFU may focus near the skin surface. The gel applied to the skin for HIFU treatment is designed to conduct sound from the probe, which is different from the purpose of the gel for IPL and radiofrequency treatment. It is desirable to use the procedure with uniform irradiation and heat distribution because excessive heating will cause skin burns. To avoid excessive accumulation of heat in the skin, HIFU irradiation should be performed once, then in a different location and then again at a later time. Twisting the linear probe may increase the risk of burns due to uneven heat distribution. In addition, pressing the probe hard onto the skin reduces tissue thickness, resulting in the increased risk of damaging deeper tissues.
Attention should be paid to side effects such as paralysis and numbness due to damage to the facial nerve or trigeminal nerve. The facial nerve exits between the superficial and deep lobes of the parotid gland and runs peripherally in a shallow layer. The marginal mandibular branch of the facial nerve runs along the lower border of the mandible and then crosses over the facial artery heading slightly upward. HIFU irradiation of this area may increase the risk of nerve damage. Figure 11 shows an echogram of the preauricular region of a woman in her 20s. The distance from the skin to the surface of the parotid gland (SMAS) is between 4.0 and 4.5 mm. As irradiation to a skin depth of 5.0 mm or more can damage nerves in the face, body probes should be avoided. For thin and elderly patients, short focal length cartridges should be used in HIFU treatment because these patients have even thinner subcutaneous tissue.

Figure 11. Echogram of the preauricular area in a woman in 20s female
Operators should be aware of the potential for damage to the trigeminal nerve. Especially in the forehead, where subcutaneous fat is thin and in close proximity to the bone, numbness may occur during HIFU irradiation. Care should be taken in relation to the course of the supratrochlear and supraorbital nerves to avoid irradiating these nearby regions. In addition, the following areas should be considered: the area around the infraorbital foramen, through which the infraorbital nerve passes, and the mental foramen, through which the mental nerve passes. Care should be taken not to injure the medial brachial cutaneous nerve when using HIFU to reduce subcutaneous fat in the medial upper arm. Patients may complain significant discomfort when numbness persists in the medial upper arm. To avoid complications (Figure 12), it is important that physicians performing the procedure have a thorough knowledge of facial anatomy and fully understand the mechanism of HIFU.
Figure 12. Points to avoid complications